Gender nonconformity is the second most popular search term that leads people to Science of Eating Disorders. (After “science of eds” and beating “science of eating disorders”.) Not far behind are variants of “FtM/MtF/transsexual/transgender” combined with “eating disorder/anorexia/bulimia”. That’s telling. It means there is little information on this topic. And it is not just that there’s too little information available to the public – there are only a handful of published studies in the peer-reviewed literature.
One study (which I discussed in my previous post: Gender Nonconformity, Transsexuality and Eating Disorders) published by Vocks et al (2009), compared disordered eating patterns, body image disturbances and self-image scores among trans women and men (131 participants in both groups) and cis female and male controls as well as to females with eating disorders.
Overall, they found disordered eating patterns reported by trans women and trans men were in the middle of those diagnosed with eating disorders and non-ED, cis controls. More specifically, trans women individuals had more severe disordered eating pathology than both female and male control groups, whereas trans men individuals reported higher levels of disordered eating than male controls but were similar to the female control group.
Several hypotheses have been raised to explain these (and similar) findings. I discussed them in my previous post, but I’ll briefly mention what I think are the two main explanations: firstly, disordered eating patterns might be used to suppress secondary sex characteristics for both trans men and women, and secondly, disordered eating might be a way to deal with the stigma, poor self-esteem, negative self-image, perhaps abuse and/or isolation that many gender nonconforming and transgender individuals face.
But those are just hypotheses, based on the authors’ own ideas and through interviews reported in case studies. Monica Algars and colleagues wanted to evaluate trans men’s and women’s’ “own understanding of [the] underlying causes.” What explanations and reasons did trans men and women participants provide for their eating behaviours and, if applicable, how did it change after gender reassignment treatment.
Algars interviewed 11 trans men and 9 trans women adults (age range: 21-62). The table below, taken directly from the paper, summarizes several characteristics of the sample. Please note that the names of the participants have been changed to protect their identity.
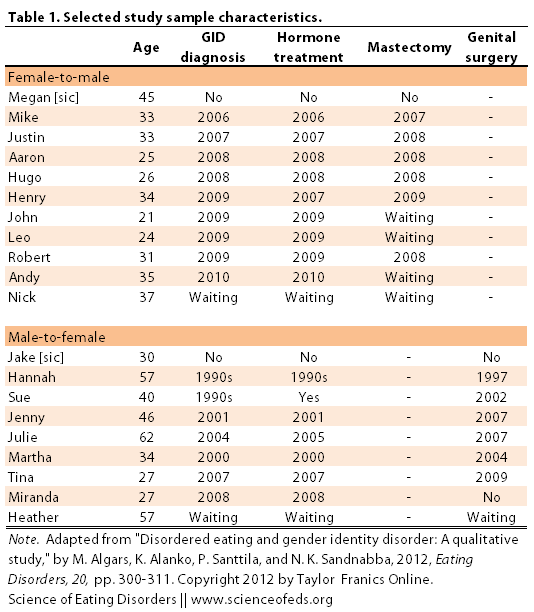
I removed the BMI values (self-reported) from the table below because I don’t think it is too important. (The average BMI of all participants is in the overweight category.) There were no differences between the groups in BMI or the Eating Disorder Inventory-3 (EDI-3) scores. Fourteen out of the 20 participants reported a history of disordered eating (70%).
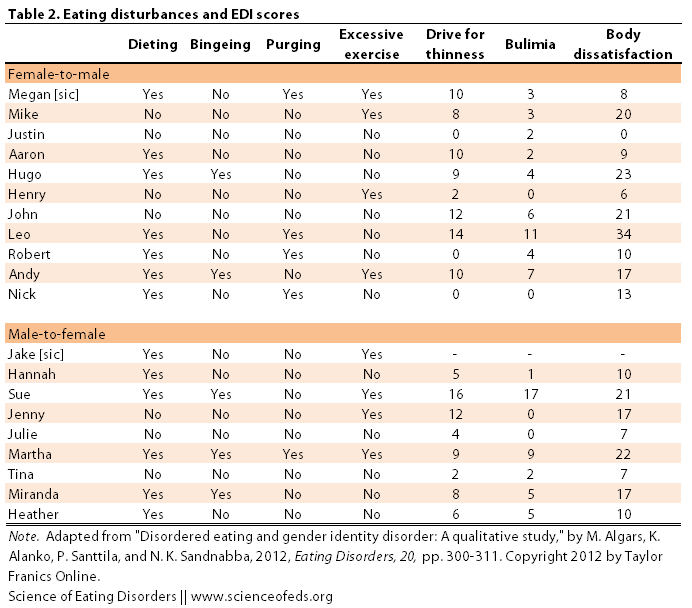
The table below, again copied directly from the paper, summarizes broad eating disturbances experienced by the participants along with their EDI-3 scores. I am not sure what the EDI-3 scores would be of a non-eating disordered female, for example, so it is difficult for me to compare, except within a group. What are the EDI-3 scores for a non-ED, cis female, non-ED, cis male, and cis ED female and male (for bulimia and anorexia)?
Although Algars, in the discussion, mentions that the “current mean EDI-3 scores on the subscales Drive for Thinness & Body Dissatisfaction were comparable to that of adult women not suffering eating disorders. Nonetheless, a within-study control group would be really helpful.
Algars and colleagues identified nine themes (organized into three “higher -order constructs”) that came up through-out the interviews. (Algars et al used grounded theory coding to analyze the interviews.)
The three higher-order constructs were: the nature of disordered eating, the perceived cause of disordered eating and the impact of gender reassignment on disordered eating.
DISORDERED EATING
In terms of disordered eating, the majority of participants reported dieting (65%), 25% said they’ve experienced bingeing, 25% engaged in purging behaviours and 40% reported excessive exercise. Note, the percentages don’t add up because one participant could have experienced all four disordered eating behaviours (or three or two or none).
The descriptions of the disordered eating behaviours are indistinguishable from diagnosable eating disorders – at least in the Algars et al paper:
dieting: ... keeping track of and restricting calorie intake, only eating certain foods, avoiding situations in which people eat, purposefully maintaining an abnormally low body weight, and weighing themselves several times a day …
bingeing: … eating large amounts of food in a short time, being unable to stop eating although they felt sick, and feeling that they could not control their eating …
purging: … purging after binge-eating, while others also had purged after eating only small amounts of food. One trans male participant reported chewing and spitting …
excessive exercise: ... bike at least xx km every day … amenorrhea due to excessive amounts of exercise
PERCEIVED CAUSE OF DISORDERED EATING
Participants that reported instances of disordered eating explained their thoughts about the underlying causes. Five participants (four trans males and one trans female) reported engaging in disordered eating patterns to suppress their biological sex (reduce femininity or compensate for masculine features, such as height). I think this is really important information, so I’m going to be quite liberal in lifting up quotes from the paper:
Andy: The background of that crazy weight loss was that my curves would disappear. They have always felt disgusting, for example my hips and my breasts.
Aaron: I felt like I wanted to diet my gender away completely, or, like, dispel it altogether. I still feel like that sometimes, that I have to diet, because otherwise I’ll start looking like a woman again.
Robert: Weight gain would have brought forth my feminine figure, which was disgusting to me. (. . .) I was so skinny that people asked me if I was sick or something, because I wanted to keep my body’s femininity at a minimum, so the fat wouldn’t distribute to feminine places.
Others – three trans female and one trans male participant – reported using weight loss to accentuate their gender.
Martha: I thought that because I was a woman I had to look good, to look more like a model. I just felt a lot of pressure to be thin all the time. I wanted to be smaller, more delicate. In my opinion it is connected to being a woman.
Heather: In general, women are more slender than men. It is easier to make a man’s body look feminine if you’re a bit thinner. ( . . . ) When I was thinner it was nice to see that I had a waist.
Mike: [After losing a lot of weight] I could buy pants at the men’s department, and they fit in a certain way, the right way, as I see it. And also, I felt strong, which I perceived as masculine.
And yet for others, disordered eating served other emotional and psychological purposes, including self-control, managing feels of inadequacy and isolation, desire for autonomy and freedom, feeling that they did not deserve to eat, that it made “sexual situations easier,” and helped them manage stress.
IMPACT OF GENDER REASSIGNMENT ON DISORDERED EATING
Out of the participants, 16 had undergone some kind of gender reassignment or treatment to facilitate transitioning into their desired gender. Algars and colleagues explored the effects of this transition on disordered eating behaviours. Four participant felt that the changes were for the positive whereas two experienced negative changes due to unwanted weight gain (the result of hormonal therapy):
Robert: Until I received hormone therapy, I controlled what I ate. (. . .) Now it doesn’t matter if I gain weight, I suppose it accumulates in different places now. The fear of weight gain, or fear of femininity, is not an issue at all anymore, that’s all gone.
Megan [trans man]: After my breast reduction surgery I gained some weight, but I was only happy about it. I could imagine being a fat man, but I could never be a fat woman. There is a huge difference.
Interestingly, Julie felt almost the converse to Megan:
Julie: Immediately [after the operation] I wanted to join the other women in the sauna, even completely undressed. Somehow I tolerate it much better now, even if someone would say something about my flab, it wouldn’t feel as bad as when I was a man. I feel like I am myself now, even with my fat. Maybe I’ve gained some kind of self-confidence.
Case studies and qualitative approaches are insightful and often fascinating, but a sample size of 20, of course, is limiting. Moreover, the sample was not random (participants could have been attracted to take part in a study due to their previous experiences with disordered eating) and all reports were from memory. Thus, the extent to which this is representative of the larger trans community remains to be seen.
Despite this, Algars’ study highlights the need for more awareness (and understanding) of pertaining to the trans community, as well as a need for specialized treatment approaches “to develop prevention and intervention measures” for disordered eating in this population.
There is a need. As one tumblr blogger put it, when linking to my previous post on eating disorders in trans/gender nonconforming individuals:
“If there were a treatment center that specialized in transgender issues, I’d be there in a second.”
(Note: I noticed that my last post on this topic was shared on a particular tumblr blog along with the comment that the terms I had used in my post were not always correct. I inquired about the mistakes, but unfortunately did not get a response. So, if I misused or conflated terms, please let me know! I am going based on information on-line, like this. But let me know if I am messing things up and I’ll correct it.)
References
Algars, M., Alanko, K., Santtila, P., & Sandnabba, N.K. (2012). Disordered Eating and Gender Identity Disorder: A Qualitative Study. Eating Disorders, 20 (4), 300-11 PMID: 22703571
There’s a term for ‘non-trans’: cisgender/cissexual. ‘Desired gender’ might bother some, since it implies that they want to be another gender rather than actually *being* that gender, since gender is an identity separate from sex, but transsexuals modify their bodies so their bodies are congruent with how they feel. ‘Biological sex’ would make more sense than ‘biological gender’, since in gender studies and stuff gender is seen as distinct from sex, not a synonym for it. It’s pretty difficult to use trans terminology that offends no one. From autumn-and-eve’s tumblr: ‘Terms cis people need to stop using to describe trans women:
Biologically male
Male-bodied
Male at birth
Gender-variant
MtF
Any transmisogynistic slur
XY-chromosomed or anything referring to chromosomes
Terms you should use:
Coercively Assigned Male At Birth (CAMAB)’ I’ve seen mentions of CAMAB/CAFAB being appropriative of intersex terminology, though.
Great, thanks Sarah! I’ll change those in the post. I will use MtF and FtM because it is quite common. Is there a consensus that these terms shouldn’t be used? I can see the objection to them.
The “desired gender” and “biological sex” are terms I lifted from Algars et al. They also didn’t sit well with me because of the implications, so I’m not sure why I used it :S – oh well, fixed it now! Also foolish of me not to use cisgender/cissexual, I’m fully aware of those terms… Unfortunately these things are automatic for me (yet).
Thanks 🙂
If you want to be safe you could just use ‘trans woman’ or ‘trans man’. If only everyone understood what those terms meant.
Yes, but I’m afraid some people might be confused.
Heather (MtF): In general, women are more slender than men. It is easier to make a man’s body look feminine if you’re a bit thinner. ( . . . ) When I was thinner it was nice to see that I had a waist.
This comment certainly resonates with me. I dont want to feel big, men are big, women are not. It is definetly more feminine to be small and you definetly have a more feminine figure. The less I weigh, the more feminine and female I appear. Proud to achieve a BMI under 17.
Thank you for your comment Amber. I’m glad that you could relate to some of what was said. My goal in putting this info out there is for this very reason: So that others may perhaps feel less isolated or alone with respect to their feelings and experiences.
Please, if you can, to stay safe, as far as weight loss/dieting is concerned.
I am the one thanking you. I thought I was alone. I have never met or spoken to a trans woman who felt about food the way I do and thought I was alone. I transitioned later in life, food was never an issue for me until I changed. It was my doctor who brought this to my attention. I am proud and think I look great, but its like a drug. Im not loosing weight anymore but it is hard work. I had always thought anorexia was something teenage girls had, not trans females and defeintly not over 40. From what little I have been able to find it seems more common amongst trans men than trans women. I am right? Do you know why?
“From what little I have been able to find it seems more common amongst trans men than trans women. I am right? Do you know why?”
Honestly, there is just so little information on this that isn’t anecdotal that it is impossible for me to say. From the handful of papers I read, my impression is that the types of eating issues may just be different among trans men and women (e.g., gaining weight vs losing weight). I can try looking in other databases for any studies on this but I doubt there’s much, if anything, on frequency and types of eating issues… anything more than just qualitative research.
Well it makes sense that a trans man woul d be oriented towards putting on weight so as to more closely conform to a male ideal. I wouldnt be surprised if lots of them work out and lift weights to develop muscle mass. I just never thought about it. But that is like anorexia in reverse from how we usually think about it. I suppose it is the unhealthy obsession with weight that is at the heart of it. I still have that, weighing yourself 20 times a day is tedious.
I really appreciate the work you have done though. People often see trans people as being uni dimesional as if being trans is all they are or there is to know. Not true, of course and nice to see someone who sees us as real people with real issues.
Hi Amber,
I just sent you two papers that may be of potential interest regarding eating issues in trans people.
Tetyana
Hello! There is indeed a burgeoning recovery resource for trans* people struggling with EDs! T-FFED: Trans* Folx Fighting Eating Disorders is the first grassroots, trans*-focused, affordable eating disorder recovery initiative to address the underserved and under-researched needs of transgender, genderqueer and non-binary people who disproportionately struggle with eating disorders and body image issues. T-FFED aims to produce multi-day and digitally accessible pop-up events (featuring workshops, support groups, nutrition, healing activities, resource-sharing and toolkit building) in cities with demonstrated need, as well as train ED healthcare professionals to better understand the unique needs of their trans* clients and patients. We are also currently conducting a survey to assess/demonstrate need and receive valuable feedback from the trans* community. Please share this valuable resource and help in this revolutionary work!!
https://www.facebook.com/TransFolxFightingEDs
https://www.surveymonkey.com/s/TCGLBS8
trans-folx-fighting-eds.tumblr.com
Read both this and your previous article. I am FtM and I absolutely have had a persistently negative body image but it is not I think related to an eating disorder. Having it diagnosed as an eating disorder was disastrous. I avoided getting fat absolutely yes, because it would put fat in all the wrong places and make me look more feminine. A lot of the things I did to de-feminize my body definitely could appear to be eating-disorder-related. I was diagnosed as anorexic as a teen though I was never actually underweight at any point and never had issues with food restriction. Just have consistently been on the thin side of normal for a genetic female body, according to most medical charts.
The resulting “treatment” efforts to “cure” my supposed anorexia very nearly killed me. The intense focus on “accepting one’s body”, and “loving oneself” was devastating beyond words. I was being told I needed to accept being female, needed to embrace and love my body’s natural curves and breasts and fertility, and that was something I just could not do without losing my sanity. It felt like it was all entirely my fault for being “obsessed” with wishing my body were male and that drove me to even more extreme attempts to de-feminize my body alternating with intense guilt for not being okay with a female body.
Proof for me was hormones, top surgery, and hysterectomy have made me a lot less concerned with gaining fat. I will never love my body the way the anorexia treatment specialists insisted I needed to, but the less female it looks to me the more comfortable I am with it and that is good enough for me. I still lift weights, but that’s something that would be considered perfectly normal if I’d been born with a penis so I don’t pay much attention to those who continue to insist that it is a problem. Just as I ignore those who insist that I must learn to love my body. Perhaps if I had not been forced into treatment for anorexia, I could have come to terms with a trans*male body, but the damage done was too severe. I will be happy with some measure of comfort and tolerance, something I know I can achieve rather than the impossible ideal that was preached to me during anorexia treatment.
Having ED specialists aware of the impacts of body dysphoria seems so critically important to me, so that other people aren’t being forced into treatment programs so ill-suited to their needs that it makes the issue worse instead of better. I was lucky. It didn’t kill me, I did end up sorting things out and finding the appropriate solutions to my body image issues, but I wish my survival had not depended quite so much on luck.
Thanks so much for your comment Pixie. I completely agree with you 100%: Tx programs and ED “specialists” need to be aware of these issues. If I am reading your comment correctly, it seems you don’t feel you had an ED? Do you think it is hard to sometimes separate whether food/eating/weight issues in trans folks are due to underlying eating disorders and require ED treatment or are due to body dysphoria and would be better resolved with hormone and or surgery treatment?
I generally think the whole “love your body” crap is questionable for cis folks, too (why not just “tolerate” your body, or you know, focus on non-physical attributes? “love” is such a tall order sometimes! I also hate that that rhetoric ignores that it is probably harder to love your body when you don’t fit a stereotypical ideal of “sexy/pretty/attractive”), but I think, as you mention, it can do a LOT more damage when it is preached to individuals with gender dysphoria.
I am glad everything is working out for you and that you’ve found the hormones and the surgeries to be helpful. That’s so important :-).
Thanks again for the comment :-).
Those ones who preach love your body clearly don’t understand what makes someone anorexic. It’s s lot like being transsexual, lots of opinions and ideas from people who have never had either condition. They talk about these conditions like they are a mental flu and they have the cure.
It’s sad really. Lately we are getting popular and all sorts of people who know nothing talk a lot. I suppose it’s some kind of improvement? Now we are interesting additions to friend collectors instead of just being freaks.
As for the man improperly diagnosed, it should serve as a lesson. These riff raff psycho babble fools can do a lot of damage. Know yourself, know that to the bone, become an expert in it. Don’t rely on the advice of others in these matters.
Mean while I continue to have weight issues and am loosing weight steadily with a bmi around 15 now. And that will end when I’m ready, or pass, but loving my quasi female body is not in the cards.
“As for the man improperly diagnosed, it should serve as a lesson. These riff raff psycho babble fools can do a lot of damage. Know yourself, know that to the bone, become an expert in it. Don’t rely on the advice of others in these matters.”
Really bad advice, that. I was 15 with the maturity of a 10-12 year old at best when they first diagnosed me with anorexia. It wasn’t my fault, I did nothing wrong. The point is that the professionals need to know and understand better, not that kids need to be their own therapists.
To be clear. I was talking about adults, not children. That is an important distinction.
Eating disorders can be serious, they have health consequences and in extreme cases people die from them. But it’s not common and it takes a very long time.
There is a world of difference between the thinking of a mature adult and that of a 13 year old. By any standards I am very thin now, but even after loosing one half my body mass my blood work and general health are fine.
So my advice is good and I should add that I am qualified to say so having an MSW with a major in gender studies. I guest lecture on the subject as well. I did not realise I had to add that children are not responsible for their own health care. I thought that was obvious.
Yes, you are right. My GID is just as serious of course. Current transition options may not be enough to keep me alive. But I think it was always just that, not an eating disorder.
It seems to me that unless the eating disorder is immediately life threatening, that treating the GID first makes a lot more sense. Doing otherwise seems too much like having a leaky water pipe and mopping the floor repeatedly instead of fixing the leak. I don’t think it would be possible to know if the eating disorder is its own thing or just caused by GID until after transition.
But although I know my own self very well, I don’t know how it is for anyone else and I don’t know much of anything about eating disorders so I could certainly be wrong.