My psychiatrist once compared my life to Dexter. He said I was living a double life. It was the summer before my final year in undergrad and I was working in a neuroscience lab. Yet things were so bad that at one point I was very close to quitting and doing Day Program treatment. (I didn’t, and things ended up getting better, thankfully.)
This post is going to be more personal than most. One, I can relate well to the topic. Two, I feel that I can give voice to it under my real name. (As opposed to just discuss it abstractly, or anonymously. There’s nothing wrong with being anonymous, but I feel that, for many reasons I am in a position where I don’t feel I have to be anonymous anymore.)
I think this is important because there are a lot of myths that surround eating disorders and those who suffer from them, and I want to do my part in crushing those myths. Moreover, while restrictive anorexia nervosa is often, at least partly, associated with positive traits like self-control, bulimia nervosa (rather, bingeing and purging more broadly) is never associated with anything positive. Not eating is one thing, but eating and throwing up is quite another. It is dirty. Wasteful.
Bulimia comes with huge stigma. This stigma is a huge barrier to treatment. Hepworth and Paxton (2007) found that “fear of stigma is the main barrier for help-seeking individuals with bulimia nervosa” (emphasis mine).
Bingeing and purging is shameful, but it is also invisible: most bulimia nervosa patients are at a normal weight. It is easier to hide than anorexia, too. (Eating and purging is often easier than not eating and making excuses for it.)
There’s also this idea that you can just stop. Hey, just eat and don’t throw up. Aren’t you smarter than that? Why can’t you do something more productive with your time. Stop being so selfish and wasting money, you arrogant girl. The world is not perfect, get over it.
There is so much stigma that in one of the studies I’ll talk about, for more than half of the participants, the study was the first time they disclosed to anyone that they had bulimia. They struggled with bulimia from 1 to 9 years (average 4). Imagine, nine years in secrecy.
Remember, too, that “bulimia occurs in all age groups, ethnic backgrounds, and social classes” (Broussard, 2005).
What I am about to write, I’m not writing to brag. It is to illustrate that there were many times I was both very functional and very sick. What I am about to write, I’m writing because I want to help end the myths that those who binge and purge are lazy, obsessed with being thin, stupid, greedy, self-centered, or arrogant. I’m writing because although someone once told me I didn’t look like someone who would have an eating disorder, I did.
(Side-note, purging often refers to vomiting as well as any other methods commonly used to compensate for bingeing, such as exercise, laxatives, diuretics, and fasting. In talking about myself, when I say “purging” I mean “vomiting.”)
I started purging at the very end of my first year in undergrad. It was at its worst in the summer before my final year and during the middle of my final year. But, I managed to finish my degree in Neuroscience with a high GPA. In that final year, I was the Review Board Manager at my University’s undergraduate journal in life science, and a News & Features Editor at JYI. That year I also applied to graduate schools in the US. I got into five schools, including two Ivy League Neuroscience PhD programs. (And then decided I didn’t want a PhD and I didn’t want to be in a long-distance relationship.)
I’ll be defending my Masters in the next 2-3 months and NSERC (Natural Sciences and Engineering Research Council, a major funding body, probably most similar to the National Science Foundation in the US) decided I was in the top 24 Masters level applicants across all fields in 2012. (I’m not, I guarantee you, but I’ll accept their scholarship.) And guess what, I was bingeing and purging a lot during the start of grad school.
If people did think something was wrong, few probably suspected how bad it was. I doubt anyone actually thought I spent most of the night bingeing and purging, and then went to the lab in the morning and did experiments all day. Few probably suspected that I purged between experiments in undergrad.
I wasn’t lazy, stupid, greedy, self-centred, or arrogant. And no one is just because they are struggling with an eating disorder. No one.
I was just sick. I didn’t know how to eat normally. I didn’t know how to eat without eating a lot. I didn’t know how to stop bingeing and purging without severely restricting. Purging was extremely calming. I liked it. A lot. It wasn’t something I could just stop by myself.
I was science student by day, bulimic, well, the rest of the time.
My experiences though, they are just an anecdote So, what I want to do is share two good papers exploring the experiences and perspectives of bulimia nervosa patients. Prior to these papers though, there was a study by Orbanic (2001) that described the experiences of six women living with bulimia.
Five themes surfaced:
- A LIVING HELL: Thoughts were overwhelming about when, what, and how much they were going to eat and how they would avoid being caught. They were emotionally and physically exhausted.
- THE PERPETUAL CYCLE: Bingeing and purging became “habitual, automatic, self-perpetuating.”
- THE RIGHT TO EXIST: Felt justified to exist only if they were thin, need for approval and self-criticism were powerful drivers of the pursuit of thinness.
- FOOD AS ANAESTHETIC: Bingeing and purging was a way to “detach from feelings and emotions”
- LIVING A FAÇADE: A lot of time and thought went into how to maintain the façade of normalcy.
I can definitely relate to all of those, perhaps with the exception of number three. Number one, and especially number two, four, and five very accurately describe my experiences with bulimia. Spot on.
Orbanic also found “that bulimic women often experience a sense of “satisfaction,” “completion,” and “calm” following vomiting.”
I’m so glad to see this written. There is a common assumption that bulimia nervosa patients like bingeing but feel guilty for the food and vomit. The assumption is that they don’t like vomiting, it is just to get rid of the gluttonous binge. For me, while that was true sometimes, I actually began to like vomiting and often binged to vomit precisely because it left me feeling incredibly calm and tranquil. There were times purging was something I felt compelled to do in order to actually fall asleep. I wanted to go to bed, but, I felt I had to binge and purge, otherwise, I wouldn’t fall asleep. I would be too anxious.
Brenda Broussard, in her 2005 paper, and Gunn Pettersen and colleagues in their 2008 paper found very similar results to Orbanic. Instead of writing too much, I thought I’d make figures illustrating the main findings of the two qualitative papers (click on image to enlarge).
Broussard (2005):

SUMMARY OF IMPORTANT FINDINGS
Broussard (2005):
- Many thought their behaviours were “normal” or weren’t a big deal, but that they were afraid others would think otherwise.
- Participant thought they were often perceived as being “gross,” “disgusting,” “sick,” “repulsive” or that there was something mentally “wrong” with them.
- After vomiting, “rather than guilt, [many] actually felt “relief” or “good.” (This is similar to Orbanic’s findings.)
- The participants faced a huge internal struggle, and attempts to rationalize the irrational but overwhelming desire to binge and purge.
Pettersen et al. (2008) found different, but similar, subthemes (note the differences between the participants):
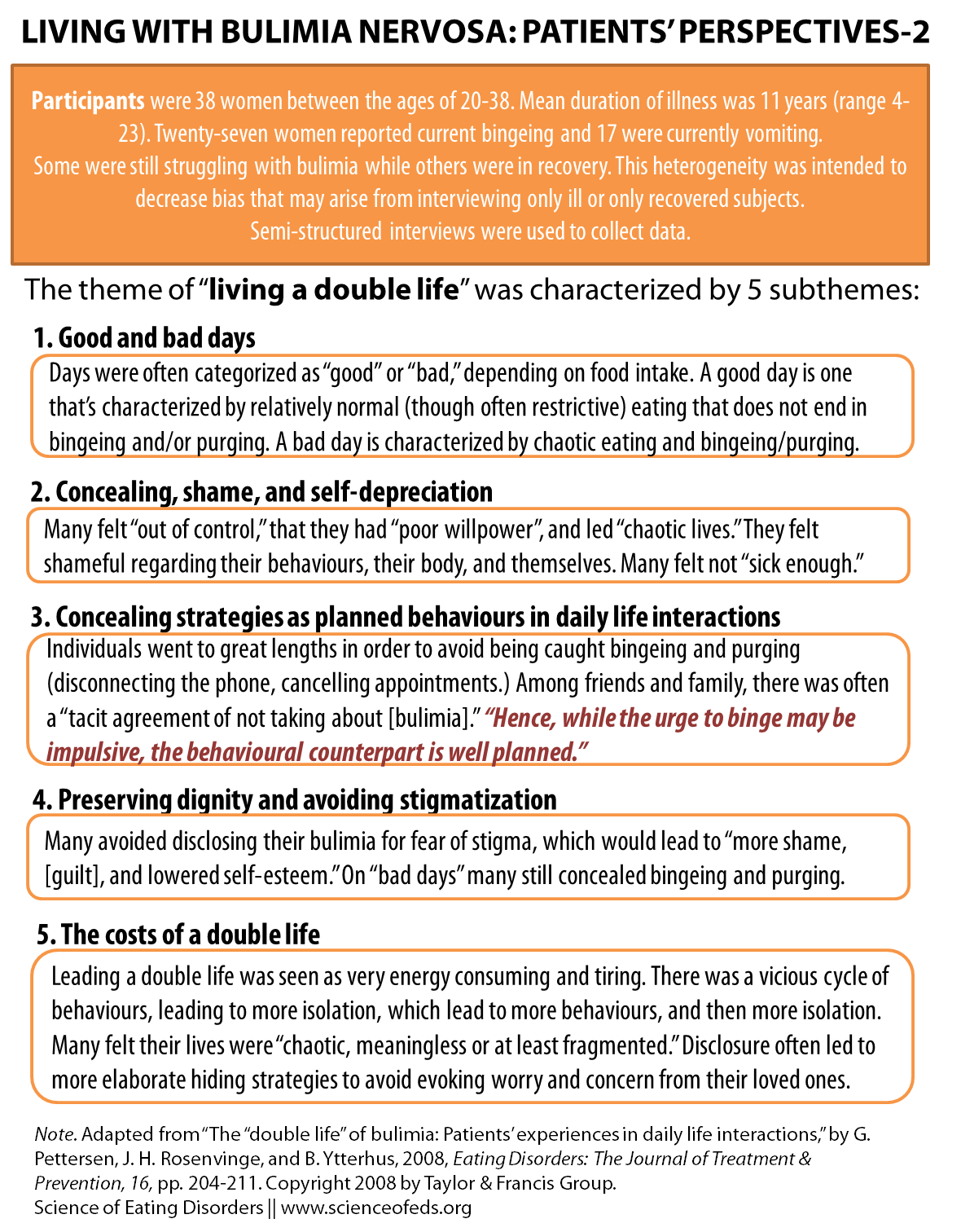
SUMMARY OF IMPORTANT FINDINGS
Pettersen et al. (2008):
- Thought often seen as being “manipulative” patients are often just trying to preserve their dignity and concealing their bingeing and purging is a way to accomplish this.
- Participants hid their behaviour for fear of shame, stigma, and negative sanctions
- Individuals who were less ashamed of bingeing and purging, and did not put as much daily effort into hiding it “may be judged as better off” (because mentally it is less exhausting).
Severity of bulimia is then not only related to psychiatric status, frequency of symptoms, or objective somatic conditions. Severity is equally a question about emotional fragmentation between shame and dignity, as well as whether the distance between the overt and the covert hampers daily life functioning.
What do these findings mean for therapy and treatment?
Pettersen writes that time should be spent both on reducing symptom frequency *and* reducing the same that it is associated with bulimia, as well as addressing the costs of the “double life.”
Broussard (a nurse) recommends studies that “involve bulimic women in a discussion about treatment strategies.” She suggests further studies should address “How can health care providers effectively address the issue of eating disorders with clients?” and “What do bulimic women think would be most helpful?”
Wouldn’t it be great if all therapists and treatment teams asked you how you feel you can be helped (particularly if you are an adult, perhaps in your mid-20’s, and have a lot of other things going on in your life, like school and work)? I can’t wait for that day.
I’m sure a lot of readers who have struggled with bingeing and purging can relate to some of themes discussed in these papers. Feel free to share your experiences, and perhaps how treatment helped or hindered recovery. (As always, you can do so completely anonymously.)
References
Broussard, B. (2005). Women’s experiences of bulimia nervosa Journal of Advanced Nursing, 49 (1), 43-50 DOI: 10.1111/j.1365-2648.2004.03262.x
Orbanic S (2001). Understanding bulimia. Signs, symptoms and the human experience. The American journal of nursing, 101 (3) PMID: 11279994
Pettersen, G., Rosenvinge, J., & Ytterhus, B. (2008). The “Double Life” of Bulimia: Patients’ Experiences in Daily Life Interactions Eating Disorders, 16 (3), 204-211 DOI: 10.1080/10640260802016696
Thank you – silence, uncertainty, shock, awe, unease, discomfort and a burning desire to hide. Emotions all evoked in reading your words. Bulimia hurts, aches and destroys a person and having beaten my previous worst binge ever by about xxxcals yesterday it stings too. xxx calories and an innumerable amount of minutes bent over the toilet to put it briefly. Knowing that I am not alone, knowing that the research supports how bonkers I feel and tells me I am not alone helps. Thank you. If you could post a miracle cure that would also be fab.
[Edited by Tetyana to remove #’s.]
I’m am writing to see if you could give a few words of advice. I’m struggling… Well dying from my ED.. Finally going to seek professional help. I am a mother of 3 children and my husband may leave me unless I can get better. I’ve been bulimic for 20 years now.. And now abusing alcohol. I’m just wanting to hear from someone who has successfully beat this. Thanks
Sent from my iPhone
Hello Candace,
I wish I could but I’ve not beaten the illness, just keep beating my worst binges and am fighting it very hard. I’m absolutely rooting for you and think talking to someone is great. I also have depression and the doctor has kept me alive.
This article made me feel a little bit more at peace… I’ve been a bulimic off and on since I was 12 (now 19) and I don’t know if I want the help… I feel like I should I know I’m sick I know what I’m doing to my body I know it’s wrong I know I don’t regurgitate nearly half the calories but I love it, it’s sick. I just don’t think anybody can help me because it’s easy to understand bulimia through a text book however it’s completely different to live with it. I purge less often now, I just try to focus more on what I eat and what I categorize as “okay” food, and if I decided to slack I just run a little more at the gym to burn off that cookie… I do have the occasional mishaps more often then not I think it’s sick because I plan it all. I buy sugar cookies the ones with the seasonal characters on them (my favorite but 110 calories for two is a no go) bake them all, eat them with 2 bottles of water and throw them all up. It’s nice because it’s sweet and if I throw up at the right time it’s the perfect texture. Sorry for the details , I’m not encouraging anything. It just feels good to be talking about it with people who understand
Wish you all luck on the road to recovery
xoxo
This made realize that there are a lot of people like me. I could relate to most of the things you wrote and what was in the studies. Sometimes I feel awful about being bulimic and want stop and get help, but I convince myself otherwise by telling myself I only want help for the attention because there’s nothing actually wrong with me. Most of the time I feel like it’s completely normal, if I eat too much or eat sugar, I can just purge and voila it’s gone no harm. I tell myself that I’m not actually hurting my body because I’m careful even though my throat gets sore sometimes. I’ve told 4 people and none of them really cared, one even asked me how I do it and if it’s hard. I started doing it two years ago because I thought it was a good way to control my cravings and get skinnier because I despise my body, but now it’s so normal I feel weird when I don’t do it. Am I actually sick? Everything I read tells me I am but I just don’t feel that way. I feel like everything is fine but I know that’s not how I should feel. I should feel bad and want help and I just don’t…
Your post really hits home with me Nicole. I’ve been bulimic for 3 months now (a brief patch 3 years ago) but consistent recently. I feel as though I’m looking forward to a binge/purge. The relief of guilt (and full stomach) after purging is almost a sense of clarity. And yet I know deep down this is not a healthy mindset and I’m obviously in a better position to prevent this bulimia getting worse. However, I just don’t feel “ill” enough for help. Then again, is this perhaps that mindset that we all take? We feel we’re in control of it. Perhaps it isn’t THAT bad. I just can’t bring myself to go to the doctors, tell a friend or even my other half. I’m at a real crossroads here…
I’ve been struggling with this since 2009. It started as something like anorexia. I was never super thin, even after losing 30 lbs, so no one thought anything of it nor would I fit the typical anorexic description. My brother had just died, and I stopped eating. It wasn’t a purposeful thing…at first. I lost weight quickly, probably because I had previously used food to cope, and such a loss of calories made losing weight quick and easy. I got addicted to it immediately. I starved myself and purged what I “had” to eat so no one would notice. Eventually, I plateaued. Once the results stopped coming, I lost all that high from losing weight. I fell right back into the depression that had started it all. That’s when my self-control did a 180, and I started binging and purging. It was happening a couple times a day for a while. I tried to get over it, but really, I just go through periods of excessive dieting and then binging. Then purging, of course. It doesn’t happen as often now, but I’m afraid every time it does. I’m afraid of what it does to my body. I need to get my wisdom teeth out, but I’m so scared to go to the dentist and find out I’ve destroyed my teeth. Each time, I am terrified of having a heart attack or dying somehow, but there is always a next time, regardless of that fear. I just don’t know how else to cope.